
I’ve been consuming what I’m now calling the “induction phase” of the Emergence Diet. In short, this is a very high carbohydrate (>400g/day) diet that is low in fat and which the protein source is mainly collagen based proteins: bone broth, gelatin, headcheese, pork rinds, pigs feet, beef tendon, etc. I am also supplementing with B-vitamins, SEA, theabrownin, r-ALA, NAC and betaine. The stated goal of the approach is insulin sensitivity.
This Twitter thread explains the collagen thing:
After only a week on this diet, I reported over at r/SaturatedFat that I had managed to reverse my prediabetes. My fasting blood glucose had dropped from an average of around 118 down into the low 90s. This seems ongoing. This morning it was 91.
But fasting blood glucose is not the ONLY, or even the best, measure of insulin sensitivity. Glucose tolerance is a related concept that asks how well your body deals with ingested glucose.
Watch The Emergence Diet Specification
How I Aced my OGTT
An OGTT is a pretty simple test. You consume 75 grams of pure glucose and then check your blood glucose 2 hours later. If your BG is above 200, you are diabetic. If it is between 140 and 200, you are prediabetic. If it is below 140, you are considered “normal”.
To do this at home, I get a bottle of glucose capsules at the drug store from the diabetic section and prick my finger every 30 minutes with a home blood glucose tester. The last time I did this was way back at the conclusion of my trial The Feasting Mimicking diet. I get a 160 ( or maybe it was a 180, I can’t remember exactly). I’d been doing a lot of fasting (which puts you into glucose sparing mode), so I didn’t expect to be super glucose tolerant. Still, it was grounds for concern.
On my current diet, I’ve been consuming ~250g of carbs in my morning meal, so I was expecting to be glucose tolerant.
This time, I got a 74. I told you I aced the test.
How I Failed My OGTT
Let’s consider the full test results.
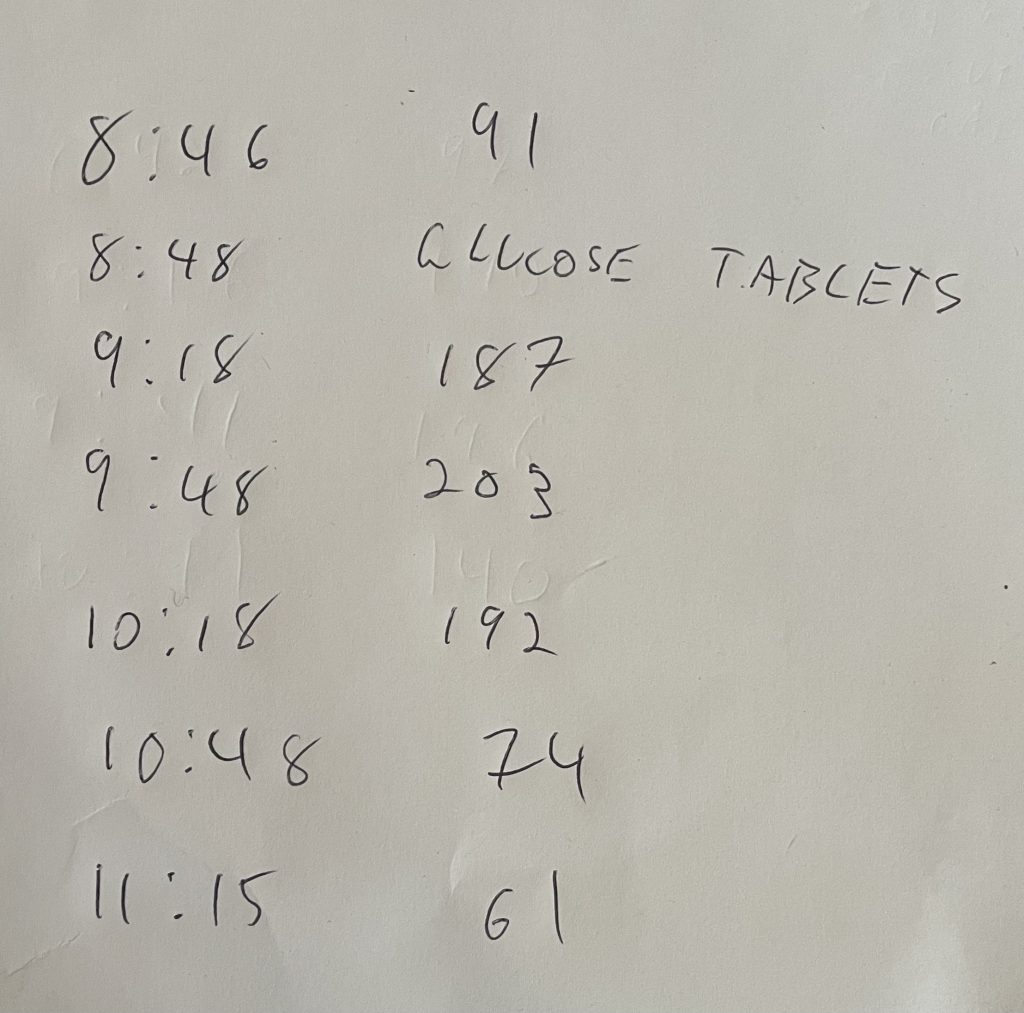
90 minutes after (10:18am) consuming the glucose tablets, my blood glucose was 192. My peak BG was over 200. 147 minutes after consuming the glucose tablets I was hypoglycemic (61).
Let’s look at my curve, that I’ve superimposed (in red) over what are considered to be diabetic and “normal” BG curves:
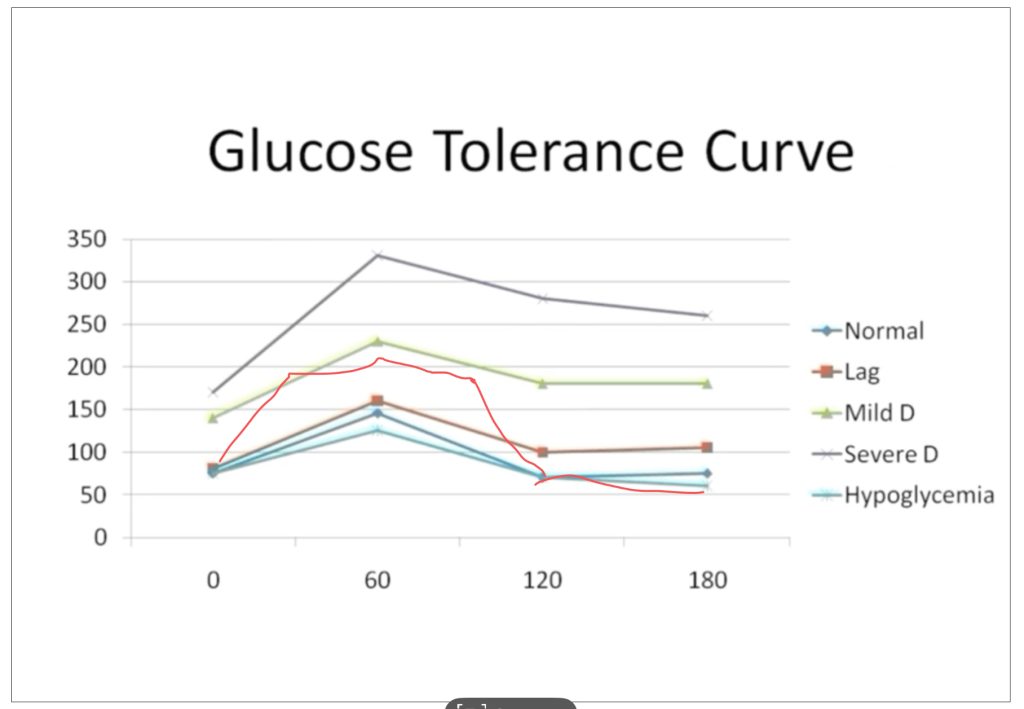
For 90 minutes I look pre-diabetic then I plunge to hyperglycemia. One of the first things lost in insulin resistance is the first phase insulin response. This is a quick hit of insulin upon food ingestion that causes the liver to start taking up glucose as it is absorbed from the intestine and before the blood glucose hits the main blood supply. From the chart it doesn’t look like I have much of a first phase insulin response. (I’m presuming here, I have no way to measure postprandial insulin.) This isn’t shocking since I already had very clear visceral obesity in first grade and that was over 40 years ago.
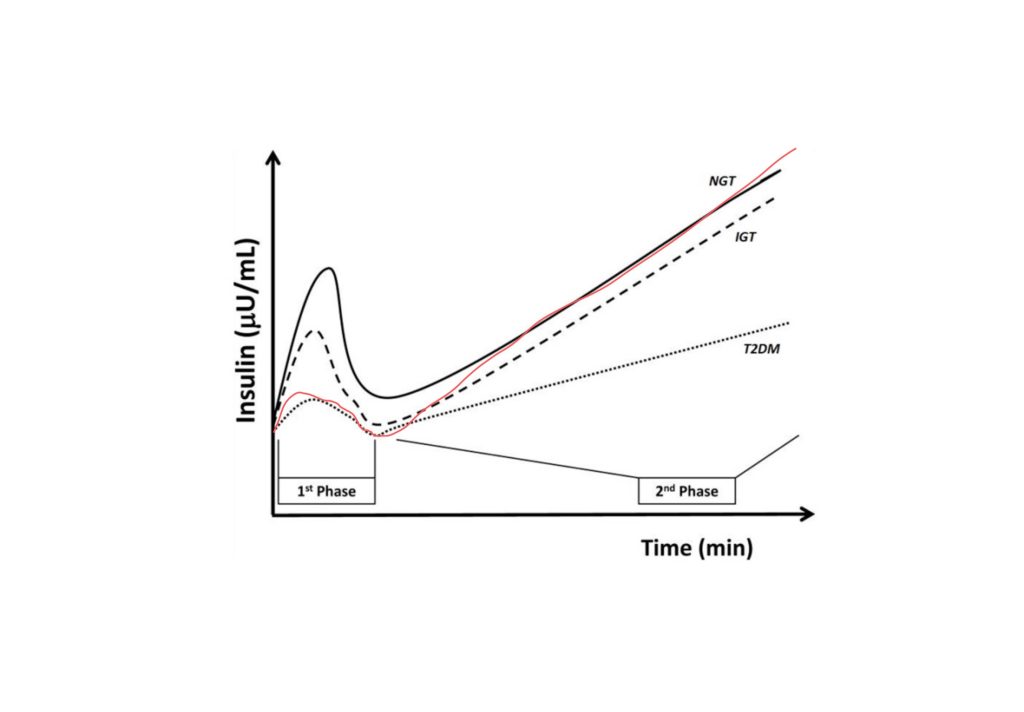
The second phase insulin response then steadily ramps up. It looks to me as if 1) I have a normal-ish second phase insulin response and 2) my body is actually burning glucose in response to the insulin!! This is, of course, the point of my new diet.
The hypoglycemia is a VERY new problem for me. I definitely felt it. Hunger, shaking hands, brain fog. I’ve been making a point of waking up and eating my pancake breakfast every day to “rev the engines”. That meal is ~250g of carbohydrate. That meal has NEVER resulted in hypoglycemia. I replaced that meal with a breakfast of 75g of straight glucose. The breakfast pancakes are made with slowly absorbed cassava flour. Slow carbs. The glucose tablets go straight into the bloodstream, causing a blood sugar spike and an insulin over-response.
The Effect of NAD+ on Blood Glucose
The reason that obese humans often are slow to switch on carbohydrate metabolism is that their mitochondria have a buildup of acetyl-CoA and a high ratio of NADH/NAD+. Both of these things inhibit pyruvate dehydrogenase (PDH): the enzyme that limits the rate that you can burn carbohydrate.
I recommend a supplement called r-ALA. The ALA stands for alpha lipoic acid and it is worth paying extra for r-ALA vs regular ALA because regular ALA can cause brain fog. r-ALA is taken into your mitochondria where it converts NADH to NAD+. Lowering the ratio of NADH/NAD+ allows you to burn glucose again by uninhibiting PDH (among other things). I normally take 480mg of r-ALA with breakfast along with a B vitamin supplement that provides 50mg of niacinamide (NAD+). I wondered if the supplements would lower my blood glucose area under the curve by supplying NAD+.
On a different morning, I did another OGTT. Grain of salt here. I did this one time each way. This needs to be repeated. To this end I am working on obtaining a continous glucose monitor to measure my BG response to a “standard challenge meal”, which will be the pancake meal I’ve already described and whose description follows below. I’m going to test the effects of r-ALA, SEA and theabrownin at least. The last two should increase NAD+ by limiting post-prandial inflammation and release of CD38.
Here was the result:
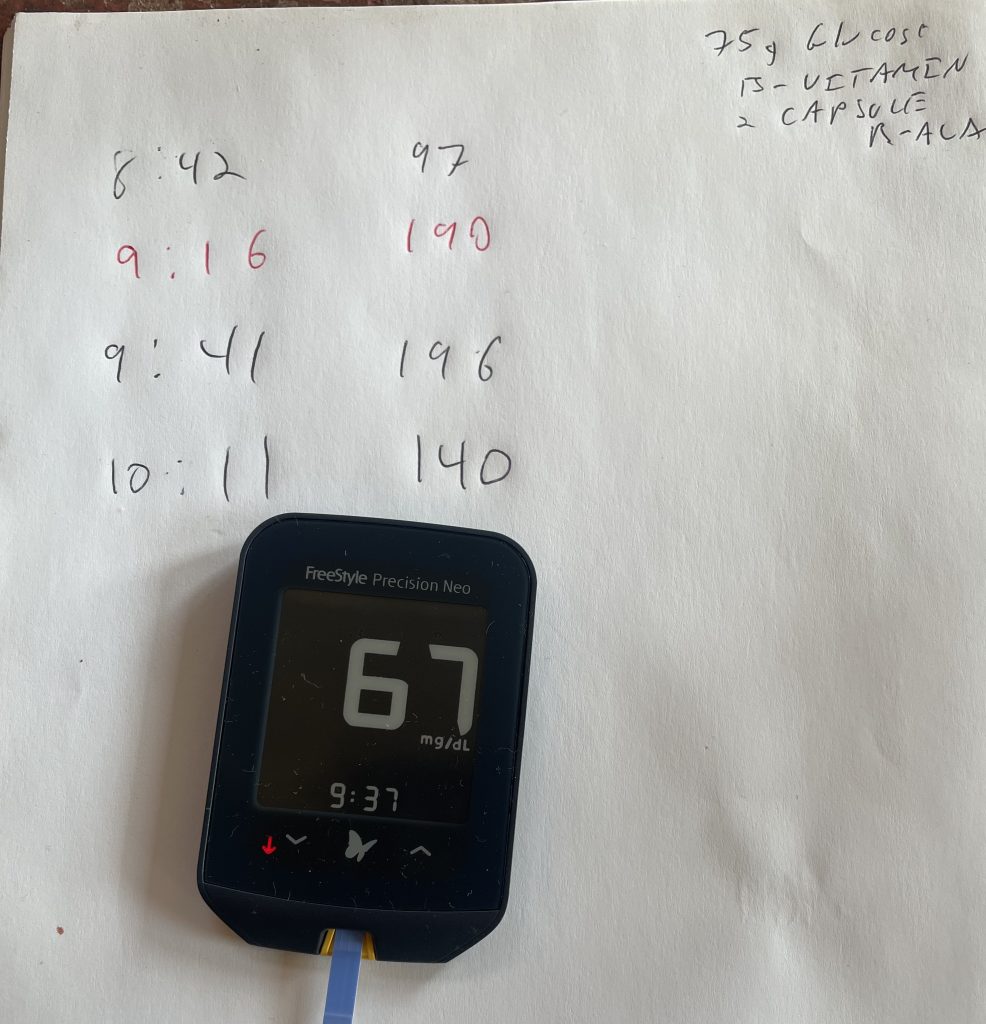
My fasting BG was high because I’d had pretty severe insomnia the night before. Late October is insomnia season. I considered not doing the trial that day at all for this reason, but there I was with the glucose tablets. I forged ahead.
The area under the curve with r-ALA and niacinamide is significantly lower. The 90 minute mark was particularly different between the two trials: 192 without r-ALA and 140 with. This is confirmation (again, this needs to be repeated) that one of the big things holding back our ability to burn glucose is too much NADH and not enough NAD+!!
NAD+ is oxygen. We “burn” our foods, which means that we oxidize them. Except that oxygen never reacts directly with pyruvate. PDH does and this requires NAD+: the OXIDIZED form of NAD. Each pyruvate that is oxidized converts an NAD+ to NADH, which is converted back to NAD+ by the electron transport chain and this is where the electrons from the pyruvate are reunited with Oxygen. NAD+ is the middle man between oxygen and your calories.
If you increase NAD+ you can burn glucose.
Cassava Pancake Test Meal
Ingredients
Method
- Add dry ingredients to bowl.
- Whisk the gelatin into 1 cup of water
- Add the egg and gelatin to dry ingredients and combine.
- Wait five minutes.
- Add water to achieve a pancake dough consistency.
- Cook pancakes without fat on nonstick ceramic griddle.
- Top with maple syrup and fruit preserves.