
The WebMD entry on alpha lipoic acid (ALA) begins with, “Alpha-lipoic acid is an antioxidant”. ALA can in certain situations act as an antioxidant, but in general it does not act as an antioxidant. If you read my article about antioxidants you’ll know that in a redox reaction, when one thing in a reaction is oxidized the other thing is reduced. Here is the reaction of ALA with NADH1.
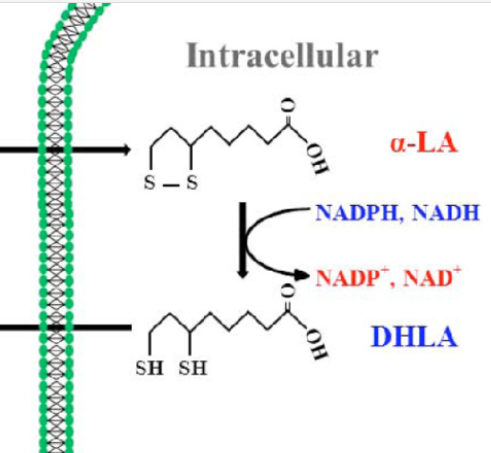
NADH is the reduced form of NAD and it gets oxidized by ALA to NAD+. ALA gets reduced in the process. ALA acts as an oxidant. It is an electron taker.
In case I stuttered: Alpha Lipoic Acid oxidizes NADH.
According to Webster’s dictionary, an antioxdant is, “a substance that inhibits oxidation”. ALA causes oxidation. By any definition, whether by the redox definition from chem 101 or by Webster’s, ALA is a pro-oxidant.
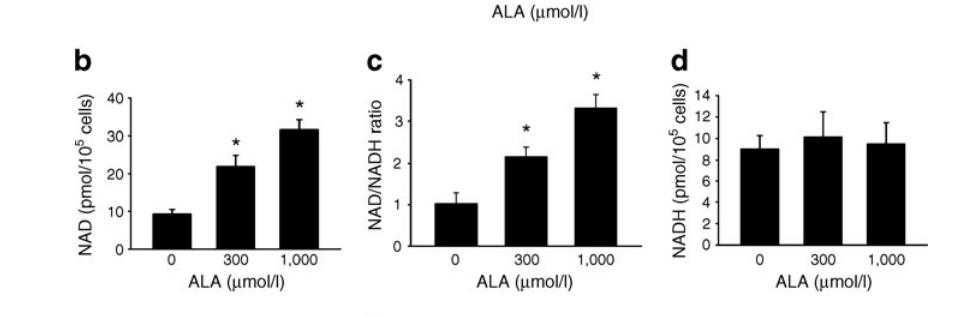
When given to cells in culture, ALA increases the amount of NAD+2, shifting the redox balance of the cell to a more oxidized one.
Just in case you missed it: ALA is a pro-oxidant.
Why do they call it an antioxidant, then?
In my previous articles I have argued that reductive stress (a low NAD+/NADH ratio) is the root cause of BOTH oxidative stress AND obesity. If you eliminate the reductive stress then you should see a reduction in oxidative stress. ALA makes the glutathione pool less oxidized and this is why it’s referred to as an antioxidant.3 It doesn’t do this directly, however, the oxidative stress is a downstream effect of reductive stress. ALA makes the glutathione pool less oxidized by oxidizing the NAD pool.
ALA eliminates reductive stress which reduces both oxidative stress and obesity.
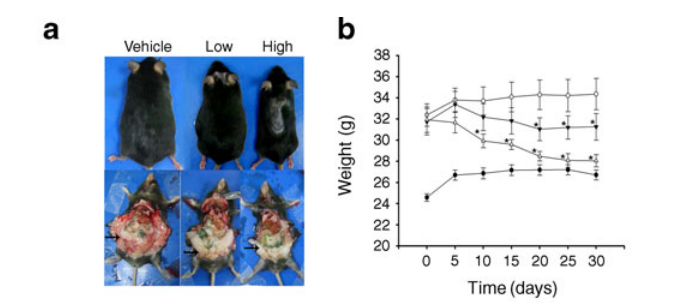
The above study2 goes on to run mice through a gauntlet of fattening processes, all of which are reversed by ALA treatment. First they make the mice diabetic using a drug cocktail of Streptozotocin and Nicotinamide. The mice become fat. Unsupplemented mice stay fat. The more ALA the fat mice are given, the leaner they become. The great thing about this experiment is that they also measured the NAD+/NADH ratio of the livers of the mice. ALA was doing its job: shifting the redox balance of the NAD pool to a more oxidized state.

Next they put mice on a high fat diet to induce obesity. No photos this time, but again the high dose ALA nearly completely reversed the obesity.

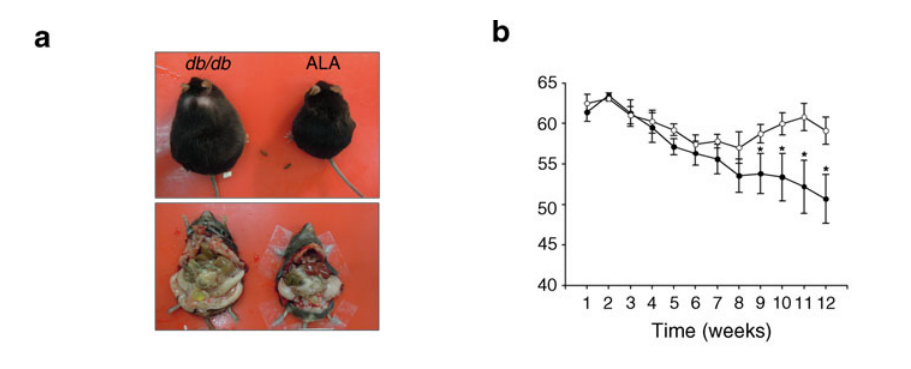
Finally, they gave ALA to mice lacking leptin: the hormone that causes satiety in the hypothalamus. I’ve written before that eliminating SCD1 can nearly reverse the effects of leptin deficiency and that eliminating SCD1 increases the NAD+/NADH ratio. Therefore both eliminating SCD1 and supplementing ALA oxidize the NAD pool. Once again, the ALA caused dramatic weight loss in very fat mice. The ALA supplemented mice lacking leptin are still plump but they have zero satiety response! My only complaint about this study is that they didn’t track calories of the leptin deficient mice.
Antioxidants should cause weight gain?
If pro-oxidants cure obesity then it’s logical to ask whether antioxidants cause obesity.
There are two possibilities here. Reductive stress in the NAD pool causes oxidative stress in the glutathione pool which exacerbates obesity by causing insulin resistance, etc. In the first case, antioxidants might help resolve some of the issues caused by oxidative stress. They might even help a bit with obesity but will not outright cure obesity.
The second possibility is that, yes, antioxidants will exacerbate the reductive stress and exacerbate the obesity.
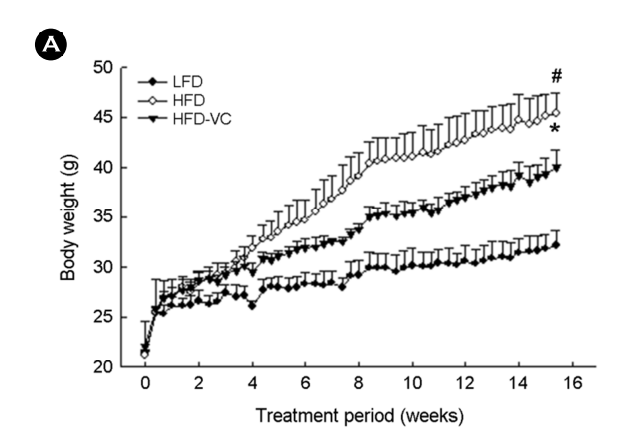
The answer seems to be that it depends on the antioxidant. Vitamin E and C are both classic antioxidants, which can give an electron. They both seem to help with the symptoms of oxidative stress. Vitamin C will reduce the weight gained by mice on a high fat diet, but they still get much fatter than control mice.4 Vitamin E typically shows no effect in combating weight gain.5
This study6 using BHA – a very effective antioxidant used in food preservation – really shows the promise and peril of antioxidants. A little bit of BHA seems to have a very small effect on reducing high fat diet induced obesity. High dose BHA exacerbates it.
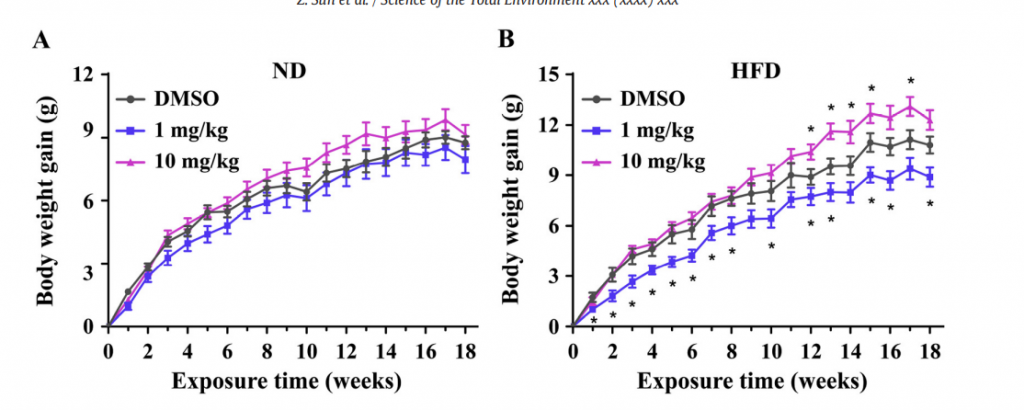
So yes, some antioxidants some of the time exacerbate obesity. Especially in high doses.
Human Trials
Luckily there is a large dataset of human trials on both Vitamin E and ALA and their effect on obesity. There are also systematic meta-analyses of these trials. I’ll let the meta-analyses speak for themselves. As to Vitamin E7, “There was no significant effect of vitamin E on weight , body mass index (BMI), and waist circumference.” As to ALA, “Alpha-lipoic acid treatment coincided with a statistically significant greater mean weight loss compared with the placebo group.”8
Oxidizing the NAD pool causes weight loss.
Supplementing ALA
I recommended taking ALA along with succinate in Obesity As a Global Succinate Dehydrogenase Activity Deficit.
First off, there are 2 types of ALA. One is R-ALA. R-ALA is specifically targeted to the mitochondria. The normal ALA is 50% R-ALA and the other 50% oxidizes NADH in the cytoplasm. The R-ALA is MUCH more expensive and it’s hard for me to justify the extra expense. I just take the regular stuff.
The amount often taken in human trials is 600mg. The “hi-dose” amount in the mouse studies that created real weight loss (200mg/kg) would be about 2,000mg in a 160 lb male after adjusting for body weight and relative metabolic rate. I’ve been taking 1200mg twice a day with good results so far.
Lipoic acid seems to be quite safe.9 It is an endogenous molecule that is taken into the cell and into the mitochondria, where it gets reduced to dihydrolipoic acid before being catabolized and eliminated in the urine. This all happens within a few hours. You can prove it to yourself because the sulfur in the lipoic acid gives you “asparagus pee”.
The largest reported side effects with lipoic acid are headaches, nausea and lightheadedness. I wrote about these effects here. I even designed an n=1 which I never did. In short, I think these effects are due to a drop in circulating lactate levels, but check out the article.
Conclusion
Reductive stress in the NAD pool is the root cause of both obesity and oxidative stress. Antioxidants can take the edge off of some of the oxidative stress, but they can’t fix the root problem. That is why such dramatic results are seen with ALA in weight loss trials in both humans and rodents and why those results are not replicable with other “antioxidants”.
Keep an eye on the blog over the next weeks, I’ll be looking at more ways to fight reductive stress! Buy some Succinade!
- 1.Park S, Karunakaran U, Jeoung N, Jeon JH, Lee IK. Physiological Effect and Therapeutic Application of Alpha Lipoic Acid. CMC. Published online July 6, 2014:3636-3645. doi:10.2174/0929867321666140706141806
- 2.Chen WL, Kang CH, Wang SG, Lee HM. α-Lipoic acid regulates lipid metabolism through induction of sirtuin 1 (SIRT1) and activation of AMP-activated protein kinase. Diabetologia. Published online March 30, 2012:1824-1835. doi:10.1007/s00125-012-2530-4
- 3.KUMARAN S. -Carnitine and -?-lipoic acid reverse the age-related deficit in glutathione redox state in skeletal muscle and heart tissues. Mechanisms of Ageing and Development. Published online July 2004:507-512. doi:10.1016/j.mad.2004.05.004
- 4.Park Y, Jang J, Lee D, Yoon M. Vitamin C Inhibits Visceral Adipocyte Hypertrophy and Lowers Blood Glucose Levels in High-Fat-Diet-Induced Obese C57BL/6J Mice. BSL. Published online December 31, 2018:311-318. doi:10.15616/bsl.2018.24.4.311
- 5.Wong WY, Ward LC, Fong CW, Yap WN, Brown L. Anti-inflammatory γ- and δ-tocotrienols improve cardiovascular, liver and metabolic function in diet-induced obese rats. Eur J Nutr. Published online October 8, 2015:133-150. doi:10.1007/s00394-015-1064-1
- 6.Sun Z, Tang Z, Yang X, et al. Perturbation of 3-tert-butyl-4-hydroxyanisole in adipogenesis of male mice with normal and high fat diets. Science of The Total Environment. Published online February 2020:135608. doi:10.1016/j.scitotenv.2019.135608
- 7.Emami MR, Jamshidi S, Zarezadeh M, et al. Can vitamin E supplementation affect obesity indices? A systematic review and meta-analysis of twenty-four randomized controlled trials. Clinical Nutrition. Published online May 2021:3201-3209. doi:10.1016/j.clnu.2021.02.002
- 8.Kucukgoncu S, Zhou E, Lucas KB, Tek C. Alpha-lipoic acid (ALA) as a supplementation for weight loss: results from a meta-analysis of randomized controlled trials. Obesity Reviews. Published online March 13, 2017:594-601. doi:10.1111/obr.12528
- 9.Cremer DR, Rabeler R, Roberts A, Lynch B. Safety evaluation of α-lipoic acid (ALA). Regulatory Toxicology and Pharmacology. Published online October 2006:29-41. doi:10.1016/j.yrtph.2006.06.004
I keep reading about the importance of not take ALA around times of exercise, so since I exercise in the morning, I have been only taking it before bed. Any thoughts on taking it before or after exercise?
Since it does drop lactate levels, which a lot of your tissues use, I could see the argument. I usually take it morning and evening.
Interesting. I was taking ALA in the morning before my workouts. I gave up using it because I was having issues.
I eat 2MAD (two meals a day). I’ll start taking 600mg in between the two meals to see if this has an effect.
Ditto. But the lactate issue may not be problematic.
Also curious about the exercise bit. Since anti-oxidant and anti-inflammatory are often used interchangably (which I remember you commenting in some of your sterculia oil stuff), I haven’t found anything definitive on what a supplement like ALA might do to the adaptations to exercise.
My guess is that since antioxidants like Vit C blunt exercise adaptations due to their attenuation of the workout induced inflammation, this wouldn’t be an issue for ALA since it would just impact the cellular energy status rather than the inflammatory milieu. But I’m also just some asshole who specialises in a completely different type of science, so I’d appreciate your take on this.
Honestly, it’s a bit hard to predict… Many of the benefits of exercise are due to the action of ROS produced during exercise. If you lower reductive stress you might lower ROS production, but it’s really hard to predict and I haven’t seen a trial on it.
Great article man, helped further my understanding in a few areas.
I just got in my ALA, succinade, stearic acid, sterculia oil, and puerh tea. I’ll let you know how it goes!
A bonus. ALA has the property of reducing lipid burden by reducing ApoB…..and possibly increasing HDL efficacy.. if you take ALA test your lipids and especially ApoB before starting. Down the line retest.
Succinade is not pleasant.
Interesting. I have a very high apoB baseline right now, and I just started succinade this week. Will be retesting everything in July. Now I’m very curious and encouraged.
Is there more nuance behind the difference between oxidizing NADH in the cytoplasm (by S-isomer) vs. mitochondria (by R-isomer)? Are there different biochemical implications – i.e. is the regular, cheap stuff potentially “better” by some mechanism than the R-ALA?
There is certainly nuance. For instance, a high NADH/NAD+ ratio in the cytoplasm drives the activity of the PUFA desaturase genes D5D and D6D, whose activity levels are implicated in the causation of diabetes. https://www.sciencedirect.com/science/article/pii/S1550413118308064
You mean more reductive stress?
Great article. But what about this study showing reduced conversion of thyroid hormones? Is it safe to use higher dose like 2 g of ALA because of this? Thank you. https://pubmed.ncbi.nlm.nih.gov/1815532/
I think this is a concern. Obviously everyone who tries it should pay attention to how they’re feeling, etc. I’ve seen enough good results in both human and animal trials that suggests that ALA is on the whole beneficial. I’ll be looking more into this angle, however.
I seem to recall hunting down the rabbit hole of thyroid hormones that one principle effect of them is to affect redox signaling, so one would have to ask if increasing ROS by this mechanism acts to trigger counter-regulation of the T4->T3 conversion via genes somehow.
The mechanism is quite complicated either way: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3872098/
That article has some interesting discussion on the general process of NAD+/NADH ratios, reductive vs oxidative stress, and ROS vs. thyroid hormones in general. I don’t see NNT mentioned anywhere, so I feel maybe that’s missing some newer nuances (it was from 2013).
An anti aging doctor was discussing Nicotinamide Mononucleotide, NMN, and NR on Joe Rogan. It gets your NAD back up to “youthful levels”. Is that something you looked into?
I have, not as much as I should yet, it seems NR is particularly promising.
1) When you say “good results so far” what results are you seeing, how long have you been taking it, and how long after beginning did you start noticing results?
2) Why did you go off the Croissant Diet since it had been so successful for you? Did you plateau? I tried to figure it out from your posts but couldn’t.
1) For a variety of personal reasons (helping a friend with back surgery, death of a friend, teaching a friend to bake cakes for her wedding), my diet has been sort of crap this winter. Too much restaurant food, too many cheat days, too much cake. The one thing I actually managed to stick to during this time was the ALA supplement (most of the time) and I didn’t actually gain any weight and my hips were down a half inch. So that’s promising…
2) I consider the Croissant Diet a big success and I think supplementing with stearic acid can be a great tool. Still, that doesn’t explain the whole why of obesity, it’s a piece of the puzzle. I’m trying to understand more of the puzzle and attack the problem from different angles. My goal is understanding, so that I can get and remain lean eating “regular” foods. Eggs and toast. Ham sandwiches. We’ll see.
That is interesting to read about S-ALA oxidizing NADH. I’m a bit confused by that because I have always heard that S-ALA actually doesn’t exist in nature. Is that a myth? Do you have a cite for that mechanism of S-ALA? I couldn’t find it in the papers cited.
My understanding is that they both (R and S-ALA) oxidize NADH but R-ALA is mitochondrially targeted whereas L-ALA is cytoplasmically targeted.
Hi, general question. Don’t the Asian countries use a lot of soy and peanut oils? Very high in PUFA, no? Why are they the skinny ones then? Thanks.
No. According to the “China Health Study”, average consumption of added oils in Chinese peasant diets is about 10g per day. The Thai rice farmers I mention in Pontzer’s Burn had macros of 84/10/6 for carb/protein/fat.
Further adding here, see John McDougall’s recommendations for diets – basically modeled after this. Yes PUFAs end up getting involved somehow but on the “traditional” Asian diets, they’re not added/supplemented and typically come from the grains/veggies in very small amounts.
ALA observation:
For about month now I have been on a high protein (minimum 60g per meal), lower fat, very low carb calorie restriction diet. I have been taking 1200mg of ALA (NOW brand, 600mg/capsule) with breakfast and a scoop of succinade with my lunch. Here’s the thing, I noticed recently that my urine stopped smelling. It used to smell for hours after I took it, now nothing. I wonder if that’s a good thing? After reading this blog entry I think I might start taking a second 1200mg with supper.
ALA, even just 600mg in AM, leaves me kinda blah – lightheaded, tired. @210lb and overweight it seems, given the study, that I would really need to ramp up the ALA consumption to see a benefit. Anyway around the side effects?
This is the most consistent statement I’ve seen about LA. In CD38 links obesity I’ve suggested other avenues to increasing NAD+: the NAD+ precursor Nicotinamide Riboside AKA Niagen and/or the CD38 inhibiting flavone apigenin.
I found ALA very interesting. I did a brief personal experiment with it earlier in the year; with 600mg of R-ALA taken all at once in the morning. The GI related side effects didn’t last long, but the one side effect that didn’t really go away and caused me to stop taking it was the severe fatigue. I mean, really debilitating, I need to sleep NOW in the middle of the day kind of fatigue. Some days I was so tired I just couldn’t do any work and the day was a write-off. I couldn’t afford to have any more such days, so gave up on the ALA. My blood glucose wasn’t doing anything unusual during this time.
Fascinating to think this might be because my lactate levels got super low and my body (? brain) just couldn’t cope. I might try again at a lower dose and at night and see how I go. Nice ideas Brad, keen to see where it’s going.
Hydroxycitric acid (HCA) in combination with Alpha Lipoic Acid (ALA) has been proposed by Dr. Laurent Schwartz as an anti-cancer compound. Furthermore, is has been demonstrated in humans that this combination of ALA and HCA is efficient against cancer cell proliferation.
Does the combination of ALA with Succinic Acid also have anti-cancer properties?
I can’t say whether ALA and succinate would have anti-cancer properties. I CAN say that cancer cells often exhibit reductive stress.
Hey Brad,
Does the ALA and succinade combo lose any effectiveness if it isn’t consumed in a fasted state?
I’m cool with the morning routine: 1200mg ALA, then scoop of succinade an hour later, then meal an hour after that. But I think I want to precede lunch & dinner with ALA and succinade too, and that’s where things get less cut and dry because I’m in a fed state more often than not. Especially if I’ve been snacking. Do I just throw ALA and succinade in on a full stomach for lunch & dinner or is that harmful/wasteful?
New to this site. Please be nice. I fast and have fixed many of my metabolic issues. Now, even at age 61, I’m down to vanity. I really want to get my waistline bulge gone. As you may know, there is a well known pattern that many fasters and keto adherents face at the endgame — they keep rebounding against a set point and migrate fat to their viscera. It is very depressing.
This ALA suggestion is very interesting. Over time, my chill during fasting has reduced. This winter, I was the warmest yet. I suspect that I’ve reduced my stored PUFA over my 5 years of fasting therapy. But 55+ years of obesity brings with it a certain resistance. My Oura ring has been tracking my temperature. I hope that we’ll see some interesting oscillations as I introduce R-αLA. The bottle from Jarrow arrived on Friday. I’m starting a 5 day fast this morning. Since Friday, I’ve seen a 0.4° increase and a 0.4° decrease. While not statistically significant, it was exciting to see the oscillation. I plan to dose with 100 mg R-αLA every 12 hours during high fat processing phases of my fast. (I’m not sure what the Biotin in all of the αLA variants does?)
Is this too low a dose? I’m happy to ramp it up but there appears to be some kind of ALA-Flu effect? (I’m not feeling anything except noting the expected change in urine odor.)
Also, if folks have protocol suggestions, I’m all ears.
Anon,
Andrew
I used to take ALA with DMSA as a chelator that could cross the blood brain barrier. When I would take DMSA I would feel amazing…clarity in vision and energy. I feel similar now when I take high doses of ALA. I used to cycle dmsa and ala because they would chelate other minerals as well. I never knew if the dmsa made me feel better because of chelating mercury like people claim or if it was actually because it was reducing my iron load. Will ala reduce iron load? Is that why some people get different symptoms? Will ALA chelate other minerals and is that a concern for long term constant use? Succinade is a no go for me as I can tell it creates inflammatory problems.
One of my favorite articles on our anti oxidant systems (SOD, CAT, and Glutathione).
https://www.sciencedirect.com/science/article/pii/S2090506817301550
The over production of super-oxide, combined with the over production of nitric oxide is a deadly combination. For someone who has the genetics for both, i take great care in managing and supporting the CAT, GPX, and SOD systems, while also lowering nitric oxide.
Though the effects of oxidizing BH4 (tretrabiopterin) into BH2 are also important given too much super oxide; bh4 is required to take phenylalinine down to tyrosine, and thus support the dopamine pathway. Its why high meat diets are hard for me – i have genetically low bh4 levels (i support with royal jelly), unless i take all the EAA’s except phenylalinine – which will scavenge the excess.
NRF2 (a master antioxidant switch) is upregulated by ALA, and in turn, NRF2 helps turn up GSR (glutathione recycling) with the help of B2. Without a functioning GSR enzyme the pool of Glutathione becomes oxidized. Lycopene upregulates GSR.
Genetic mutations in these enzymes can dramatically effect their functioning.
It is certainly true that genetic mutations can dramatically effect the function of these pathways. Perhaps a future direction of the blog will be personalized medicine, now that the first pass at the theory is nearly finished.
Brad